SLAP LESIONS
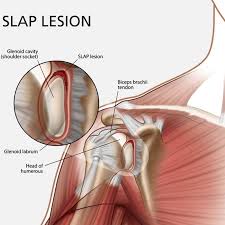
A SLAP lesion is an injury to a part of the shoulder joint called the labrum or glenoid capsule. The socket of the shoulder joint is extremely shallow and therefore to compensate for the shallow socket, the shoulder joint has a rim of cartilage called a labrum that forms a cup for the end of the arm bone (humerus) to move within.
A SLAP lesion is an injury to a part of the shoulder joint called the labrum or glenoid capsule. The socket of the shoulder joint is extremely shallow and therefore to compensate for the shallow socket, the shoulder joint has a rim of cartilage called a labrum that forms a cup for the end of the arm bone (humerus) to move within. A specific type of labral tear is called a SLAP tear; this stands for Superior Labrum from Anterior to Posterior. The SLAP tear occurs at the point where the tendon of the biceps muscle inserts on the labrum resulting in a tear at the top of the joint capsule. A SLAP lesion is as a result of an acute trauma due to overload, resulting in a degenerative lesion. The most common mechanism of injury is repetitive overload (e.g. swimmers and throwing sports) or excessive inferior traction (e.g. carrying or dropping and catching a heavy object). Symptoms of a SLAP Lesion A typical symptom of a SLAP lesion includes a catching sensation and pain with shoulder movements, most often overhead activities such as throwing. Patients usually complain of pain deep within the shoulder or in the back of the shoulder joint. It is often hard to pinpoint symptoms, unless the biceps tendon is also involved. In cases of SLAP tears with associated biceps tendonitis, patients may complain of pain over the front of the shoulder.
Treatment Options
There a four (4) types of SLAP lesions.
- Conservative management for all, but the most minor SLAP lesions are usually unsuccessful.
- Unstable (shoulder feels as though it will give way) SLAP lesions (types 2 and 4) should be repaired arthroscopically by reattaching the labrum to the glenoid.
- Stable SLAP lesions (types 1 and 3) usually respond to arthroscopic debridement to eliminate mechanical irritation is usually adequate.
- Labral lesions are often associated with a shoulder that feels unstable; this will be addressed with a graded strengthening program for the shoulder and scapula stabilisers. This should be designed and supervised by your Physiotherapist. In some cases repair is not possible and a small portion of the meniscus may be trimmed or cut out to even-up the surface.